
SonohysterographyandHysterosalpinography
Mindy M. Horrow, MD, FACR, FSRU
Director of Body Imaging
Albert Einstein Medical Center
Associate Professor of Radiology
Thomas Jefferson Medical College
May, 2011
SonohysterographyTechnique
Premenopausal: perform in early proliferative phase,days 4-10
If intermittent bleeding, clots are unavoidable
Contraindications: pregnancy, active PID, ± IUD
Pre-imaging for size and position of uterus and anyfree fluid and adnexal abnormalities
Talking to patient will help with anxiety
Ibuprofen for pain
Materials: 5F balloon catheter (prepare by flushing),speculums, sterile saline, betadine and swabs
Rescan at end, use cine and 3D, discuss results

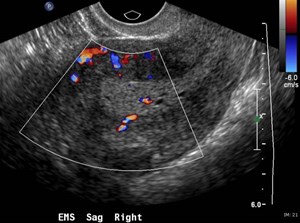
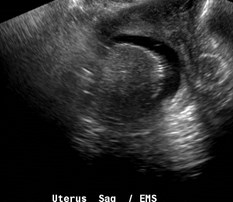
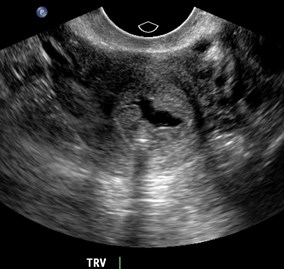
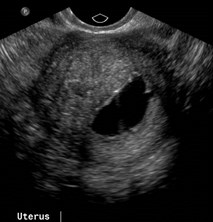
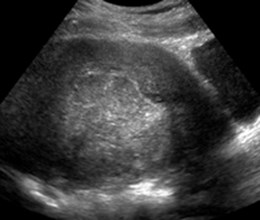
Normal premenopausal endometrium


Patient with very irregular menses
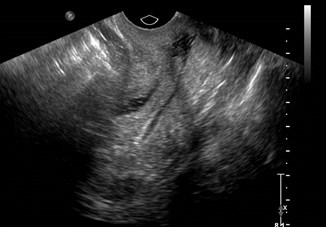
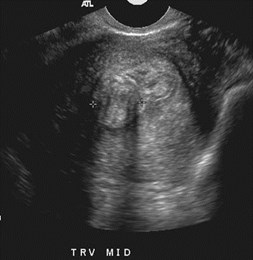
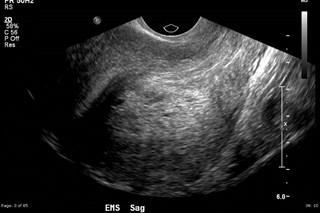
Secretory phase endometrium


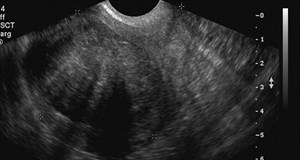
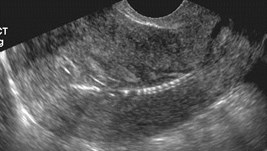
Blood clot-debris



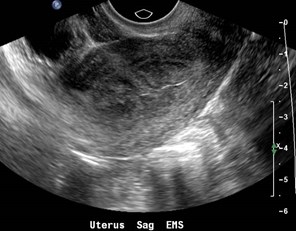
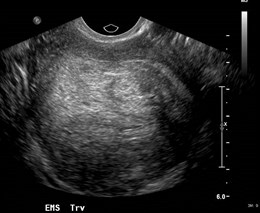
Bubbles



Poor distention
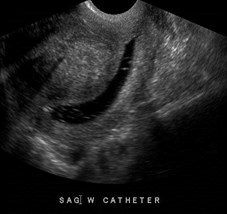
Improved distention with balloon occluding os

Fill vagina with fluid to visualizeexternal cervical os

Inject saline as catheter is withdrawn tovisualize endocervical canal


Polyps: pedunculated and broad based


Preliminary imaging
Long polyp with cystic spaces

Post menopausal bleeding

Long polyp extending into endocervical canal


Endocervical polyp
Polyps
Localized hyperplastic overgrowth of glands and stroma
Account for 30% post menopausal bleeding
Premenopausal: intermenstrual bleeding, metrorrhagia,infertility
Typical appearance: well-defined, homogeneous polypoidlesion that is isoechoic to endometrium, preserving theendometrial-myometrial interface. Often with feedingvessel
Atypical appearances: cystic, multiple, heterogeneous dueto infarction or hemorrhage

Myoma less than 50% submucosal


Menorrhagia
Intracavitary Myoma: forms acute marginswith endometrium


Heavy menses


Pedunculated intracavitary myoma
Submucosal Leiomyoma
Common source of bleeding
Premenopausal: reproductive dysfunction includingrepeated miscarriage, infertility, premature labor, fetalmalpresentation, complications of labor
Postmenopausal: 10% cases of bleeding
Advantage of SHG is depiction of percentage of fibroidprojecting into cavity (> 50% may be removedhysteroscopically)
Usual appearance: broad based, hypoechoic, solid,shadowing with overlying layer of echogenic endometriumconfirming their subendometrial location (polyps arisefrom endometrium)
Unusual appearance: pedunculated, prolapsing into cervix




Multiple polyps and a submucosal myoma


Heavy menses and inter-menstrual bleeding



Myoma
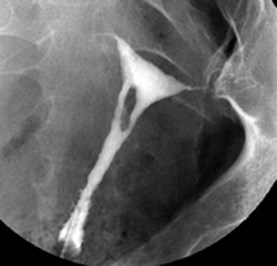
Cesarean scar niche

Heavy menses, pre-imaging, 10 daysafter onset of menses

Multiple polyps?
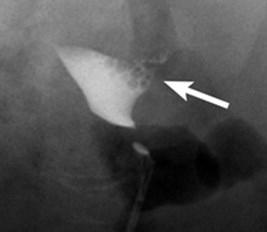
Endometrial Hyperplasia
Endometrial Hyperplasia
Caused by endometrial stimulation from unopposedestrogen
Proliferation of glands of irregular size and shape withincreased gland-stroma ratio
Risk factors similar to carcinoma: endogenous orexogenous estrogen, tamoxifen, nulliparity, obesity,hypertension, diabetes
Histologically ranges from hyperplasia to severe atypia
Usual appearance: diffuse thickening
Unusual appearance: focal abnormality that can overlapwith polyps


Small polyp and adenomyosis

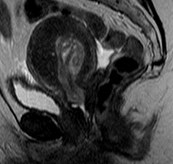
Adenomyosis
•Ectopic endometrial glands and stroma within myometriumwith surrounding smooth muscle hypertrophy
•May obscure endometrium on TVUS creating a pattern ofpseudoendometrial thickening
•TVUS findings: heterogeneous myometrial echotexture,asymmetric myometrial thickening, myometrial cysts,striations, poor definition endometrial-myometrial junction
•HSG findings: ill-defined areas of fluid intravasation,“cracks” likely represent channels of endometrial invasion,hyperechoic foci (air intravasation) that sometimes is notat actual site of adenomyosis
Verma etal. AJR 2009;192:1112



Huge polyp and adenomyosis
(notice increasing free fluid)

Small crack fills with increasing distention:
Adenomyosis



History of 3 miscarriages
Adhesions
Intrauterine Adhesions
May present with infertility, recurrentpregnancy loss
TVUS usually normal
SHG: mobile, thin echogenic bands bridgingcavity. May also be thick with poordistensibility of cavity. May be associated withscars.


Two other patients with adhesions
Davis etal. Radiographics 2002;22:803
HSG Technique
Schedule exam during days 7 – 12 ofmenstrual cycle
Anti-inflammatory meds
Contra-indications: active PID, pregnancy
Technique similar to sonohysterography,using 5F catheter with balloon
Image during filling: early, mid and late toevaluate for free spill


Fallopian tubes: interstitial, isthmic, ampullary portions

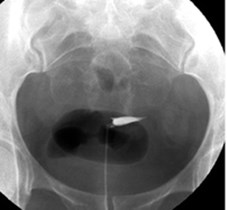
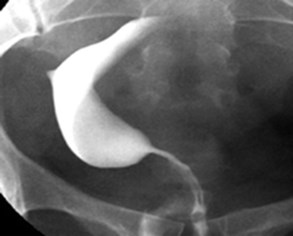
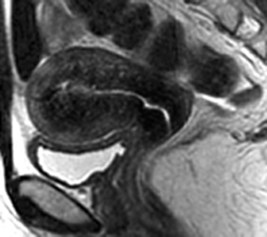
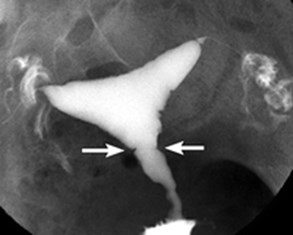
Unicornuate Uterus
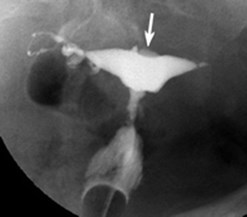
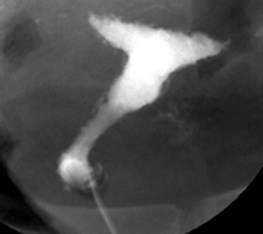
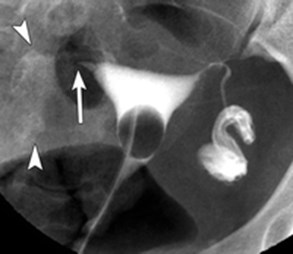
Bicorunate Uterus
Air bubbles, expelledinto fallopian tube

Uterine folds: normal variants, due to infolding of innermyometrium in underdistended uterus
Synechiae: intrauterine adhesions 2° curretage, infections.Manifest as irregular linear filling defects. Multiplesynechiae associated with infertility = Asherman Syndrome
Two different patients
Large submucosal myoma

Early filling Later filling
Small myoma better visualizedwhen uterus is less distended
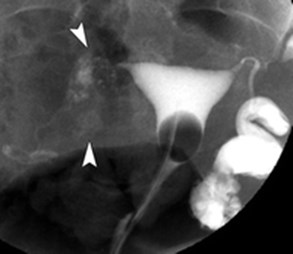
Diffuse Adenomyosis
Adenomyosis
May be imaged with HSG if nests ofendometrial tissue connect toendometrial cavity
At HSG, appears as small diverticulaextending into myometrium
More commonly detected on US or MRand is an incidental finding on HSGperformed for other reasons

Focal Adenomyosis
Cesarean section scar: can also see a wedgeshaped outpouching or diverticulum

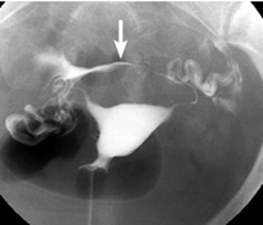
Salpingitis isthmica nodosum
SIN
Unknown etiology
Associated with infertility andoccasionally ectopic pregnancy
Appears as small outpouchings ordiverticula from isthmic portion offallopian tube
Can affect one or both tubes
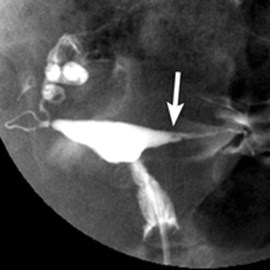
Cornual Spasm
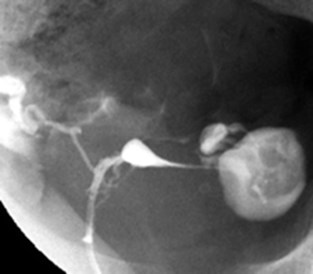
Also findings of SIN on right and hydrosalpinx on left
Spasm
Cornual (isthmic) portion of fallopiantube is encased by smooth muscle ofuterus
If spasm occurs during HSG one orboth tubes may not fill beyond isthmicportion
Indistinguishable from tubal occlusion
Can try glucagon to relieve spasm


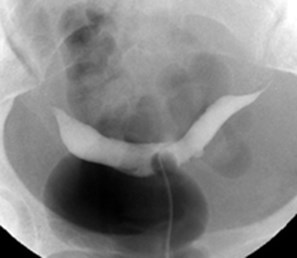
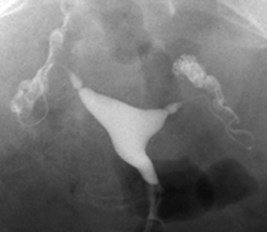
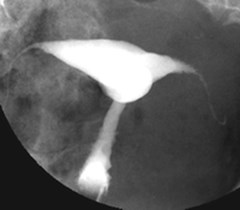
Bilateral hydrosalpinges, no free spill
Early Late

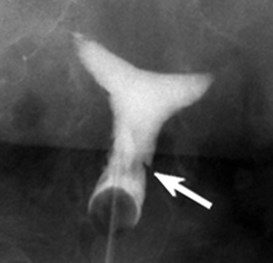
Tubal Occlusion: abrupt cut-off of contrast in isthmicportions of tubes with bulbous dilatation of distalaspects. Characteristic of surgical tubal ligation.
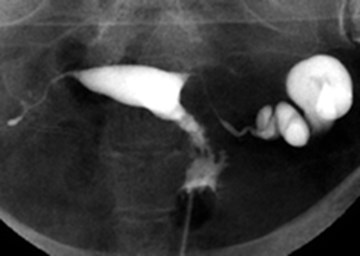
Hydrosalpinx: dilatation of ampullaryportion of fallopian tube, no spill on left,right side with prior tubal ligation
Peritubal Adhesions
Pelvic Inflammatory Disease
Chronic findings may be demonstrated on HSG
If tubal blockage is in ampullary portion, tubemay dilate, forming a hydrosalpinx.
Scarring in peritoneal cavity causes adhesionswhich prevent contrast material from flowingfreely around bowel loops, manifesting asloculations of contrast around ampullaryportion of tube
Tubal Polyp: ectopic endometrial tissue ininterstitial portion of tube. Usually asymptomatic
From: Hysterosalpingography: A Reemerging Study
Simpson WL, etal Radiographics 2006; 26:419-431

